
You know that IBS and fatigue are connected. But what about constipation? Could constipation be an early warning sign of chronic fatigue syndrome?
For those readers with CFS, I’m confident you can relate to some of the irregularities in your guts. The medical literature has documented many connections between chronic fatigue syndrome and gut issues like IBS or constipation.
What’s really going on with fatigue and your GI tract?
Is it IBS or constipation?
An unclear understanding often leads to a diagnosis based on exclusion. Instead of basing the diagnosis on the facts. In this article, we’ll explore the difference between chronic constipation and irritable bowel syndrome.
If you suffer from constipation, it does not mean that you have irritable bowel syndrome. If you have irritable bowel syndrome, it does not guarantee that you’ll have constipation.
For most of its life, irritable bowel syndrome was a diagnosis of exclusion. This means that if your symptoms didn’t fit with any other disease and laboratory tests revealed no positive findings, the doctor would label your condition as IBS.
Fortunately, in 2016 the diagnostic criteria for irritable bowel syndrome changed. Doctors now use what is called the Rome Foundation for diagnosis. The Rome criteria are based primarily on symptoms (not laboratory tests) which mean the diagnosis is still quite subjective. However, the Rome criteria are a step in the right direction for helping those with IBS get properly diagnosed.
The Rome criteria are as follows:
Rome IV
- Recurrent abdominal pain, on average, at least one day per week in the last three months, associated with two or more of the following criteria:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
- * the above must occur for the last three months with symptom onset at least six months before diagnosis
Based on the new Rome criteria, you can be chronically constipated and not have irritable bowel syndrome. In order to be diagnosed with IBS, abdominal pain must be present. That is the only difference between a diagnosis of IBS and a diagnosis of chronic constipation.
See how subjective the diagnostic criteria is?
While the diagnostic criteria have improved, we still have a long way to go before we fully understand the mechanism behind irritable bowel syndrome.
When is it considered constipation?
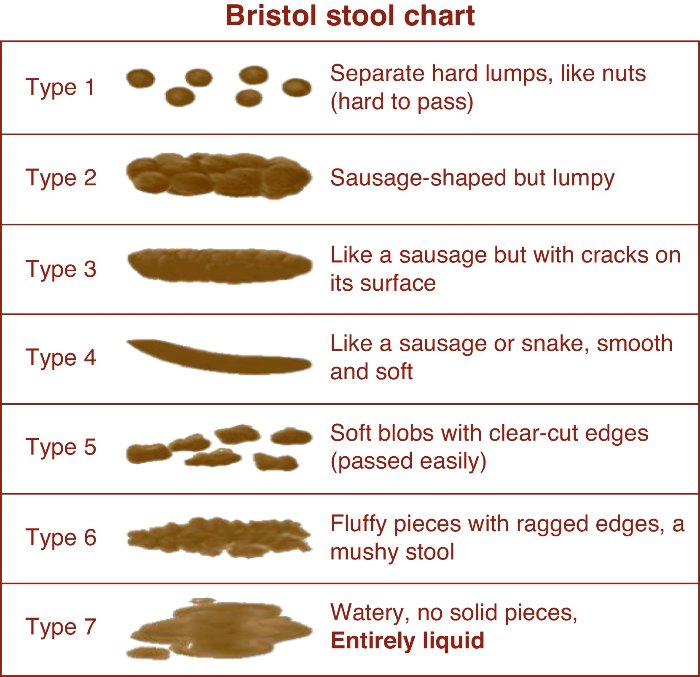 In the Bristol stool scale (image to your right), the images move from a slow transit time (type 1 and 2) to those typical of very fast transit times or diarrhea (type 6 or 7). Generally, type 3 and 4 are considered ideal for the majority of us.
In the Bristol stool scale (image to your right), the images move from a slow transit time (type 1 and 2) to those typical of very fast transit times or diarrhea (type 6 or 7). Generally, type 3 and 4 are considered ideal for the majority of us.
The general agreed upon consensus is that a bowel movement less than three times per week would constitute constipation. Please note that this is subjective; as I’m sure many readers would agree that having a bowel movement less than once per day would be considered constipation.
Additionally, the difficulty experienced with the evacuation of hard and dry stools may also constitute a diagnosis of constipation.
The different types of constipation
Medically, there are official criteria for specific types of constipation. The most common types are:
- Chronic constipation
- Chronic constipation is a common condition that is characterized by difficult, infrequent, or perceived incomplete evacuation of bowel movements. Symptoms of constipation include having less than 3 bowel movements per week, straining, hard stools, incomplete evacuation and inability to pass stool. Patients with chronic constipation do not have diarrhea unrelated to using laxatives. The prevalence of chronic constipation ranges from 2-28%. Up to 63 million people in North America meet the diagnostic criteria for chronic constipation. Epidemiologic studies demonstrate that the prevalence of constipation increases with age and is more common in women than men. (9)
- Chronic idiopathic constipation
- Chronic idiopathic constipation or CIC is a gastrointestinal motility disorder in which you have infrequent bowel movements. If the difficulty of passing stool through bowels persists for 6 months or more or keeps coming back, it is deemed as ‘chronic’. Chronic idiopathic constipation is a chronic condition in which the cause of constipation is unknown. (10)
- Opioid-induced constipation
- Opioids are a class of drugs that are commonly prescribed for their analgesic, or pain-killing, properties. They include substances such as morphine, codeine, oxycodone, and methadone. Opioids may be more easily recognized by drug names such as Kadian, Avinza, OxyContin, Percodan, Darvon, Demerol, Vicodin, Percocet, and Lomotil. (12)
- Opioids often cause constipation, or opioid-induced constipation (OIC). OIC is an uncomfortable side-effect that occurs in many patients who receive opioid treatments to relieve pain. (13)
- Functional constipation
-
Functional constipation, known as chronic idiopathic constipation (CIC), is constipation that does not have a physical (anatomical) or physiological (hormonal or other body chemistry) cause. It may have a neurological, psychological, or psychosomatic cause. (11)
-
- Irritable bowel syndrome type-C
-
IBS‑C is defined as belly pain (abdominal pain) associated with constipation. The symptoms of IBS‑C are defined as long-lasting and keep coming back. Those suffering from IBS‑C also have hard or lumpy stools at least 25% of the time, and loose or watery stools less than 25% of the time.
-
What’s the connection between fatigue and your guts?
The exact connection remains a mystery.
Fortunately, new research has illuminated a strong connection between your gut and your brain. Some writers call this the gut-brain axis. The gut-brain axis is the series of nerves the connects your digestive tract to your brain. The vagus nerve is one of the primary information highways connecting your gut to your brain.
The hypothalamic-pituitary-adrenal (HPA) axis is your body’s stress response system. Both physical and mental stressors have been found to activate the hypothalamic-pituitary-adrenal (HPA) axis. Remember chronic fatigue syndrome could be caused by chronic stress.
New understandings of chronic fatigue syndrome are viewing CFS as a chronic inflammatory condition. In response to inflammation, your body will This theory holds weight too. Stress is a form of inflammation. Under chronic stress, your body will release cells to help reduce inflammation.
When under stress, your body releases specific cytokines like interleukin 6 (IL-6). The release of these cytokines triggers the release of a hormone called Corticotrophin-releasing hormone (CRH). CRH activates your HPA axis. (1)
If you have chronic fatigue syndrome, it’s likely that your body will have elevated levels of cytokines like interleukin 6 or tumor necrosis factor alpha. With these inflammatory markers in circulation, your HPA axis will sense a stress. When this happens, motility to your GI tract is decreased. This is the fatigue-constipation connection.
Imagine you’re out for a hike. It’s a beautiful day and you’re out with friends. In this situation, it’s safe to assume your HPA is not active – you’re experiencing no stress. But then you run into a bear. High stress- immediately!
Your HPA axis springs into action releasing a cascade of hormones like cortisol and adrenaline that will enable you to run really fast. The downside to this occurrence is that it decreases motility in your gut. But who cares about pooping when there’s a bear?
This only becomes problematic when the stress becomes a long-term issue. In chronic fatigue syndrome, there are inflammatory processes (stress) ongoing for a long period of time. Like seeing a bear, this stress decreases the motility in your digestive tract. When severe, this can cause constipation.
And that is how chronic fatigue syndrome and constipation are linked!
Natural remedies for constipation
Like many chronic conditions, constipation is considered to be a result of the industrialized diet and lifestyle. A diet that is low in beneficial bacteria and fiber. Combined with a lifestyle high in stress and sedentary activities results in sluggish bowels.
Fiber
Fiber is the indigestible aspects of plants that include: cellulose, gum, pectins, and mucilages.
The current recommended daily intake of fiber is 25g/day for women and 38g/day for men. This current recommended amount is undergoing research as many believe that to be too low a level of fiber intake. Instead, ideal fiber intake is thought to be 40g/day for women and 50g/day for men.
A report from the Institute of Medicine estimated that only 3% of North Americans are getting adequate fiber intake. (14)
A study done in Brazil showed that children suffering from chronic constipation typically consumed 20-30% less fiber than their peers with normal bowel habits. Additionally, an American study showed that constipated children were consuming less than 25% of the recommended intake. Even though they had been instructed to consume a diet high in fiber. (15, 16)
Increasing fiber intake should be the first course of action when treating chronic constipation. Some of the best sources of fiber for constipation include:
- Flax seeds
- Flax seeds contain both fiber and oil which adds bulk and lubrication to the stool.
- Consume 1-3 tablespoons of ground flax each day.
- Psyllium seeds or seed husk
- Glucomannan
- Glucomannan is a highly viscous fiber from the root of konjac fruit.
- Dosing should be between 2-5g per day
Water intake
It may seem obvious that a solution to hard, dry stools is to increase the amount of water consumed. Nevertheless, increasing water intake has been shown to improve constipation.
In one study, subjects were given 25g of fiber/day. half of the subjects were instructed to drink 2 liters of water. The other subjects were given no instructions on the amount of water to consume. The group given instructions consumed nearly twice as much water as their peers (2.1L vs 1.1L). The group with increased water intake had better outcomes in both stool frequency and use of laxatives. (20)
If you are dealing with constipation, aim to consume 2+ liters of water each day.
Osmotic Agents
Osmotic agents will force retention of water in the colon. This will induce a laxative-like effect.
The most common osmotic laxative is poorly absorbed magnesium supplements. This includes magnesium sulfate, magnesium hydroxide (milk of magnesia), and magnesium citrate.
Vitamin C in the form of ascorbic acid can also help to soften the stool. The dose needs to be quite high in order to achieve this effect.
With all osmotic agents, one should carefully find the lowest dose required to soften the stool. Excessive use of these agents can create a mineral imbalance.
Botanical stimulants
Botanical stimulants contain a class of compounds called anthraquinone glycosides. These compounds act on cells in your colon causing changes in water absorption and motility. In turn, this will create a laxative effect.
Common botanical stimulants include:
- Aloes
- Aloe stimulates motility within the colon. It stimulates contractions within the digestive tract which results in an acceleration of the stool through the intestines.
- An optimal dose of aloe is the smallest dose required to obtain a soft stool. Typically, this is between 250-900mg/day. 24 hours should pass between doses.
- Senna
- a typical dose is 0.6-2g. the dose should be slowly increased over time
Physical Activity
While there is no conclusive research that proves sedentary activities cause constipation, there is certainly a strong correlation.
In one Japanese study, the addition of walking and dietary fiber from rice significantly reduced symptoms of constipation. Another study in the Netherlands instructed subjects to walk for 30 minutes each day for 12 weeks. When compared to subjects who were given no instructions on physical activity, those who walked for 30 minutes each day had a decrease in constipation symptoms. (21)
What if you still have constipation?
The above recommendations can help for generalized constipation. But when your constipation is a symptom of a more severe, underlying condition like chronic fatigue syndrome, a much more thorough investigation is warranted.
The first step you can try is the fatigue reset diet we recommend to patients. This 30-day plan will help you decrease the inflammation commonly associated with chronic fatigue.
If that doesn’t improve your symptoms, a thorough investigation of your HPA axis is warranted. Conditions like adrenal fatigue are common causes of functional constipation.
Ok, now I want to hear from you!
What sort of connection(s) have you found between your energy levels and your bowel movement!?
Click here to learn more ways to achieve a fatigue-free body!


